Indolent ulcers frequently occur in dogs and are the most common canine eye disorder seen by the UVS Ophthalmology service. They are also referred to as spontaneous chronic corneal epithelial defects (SCCEDs), persistent corneal erosions, non-healing ulcers and Boxer ulcers. While indolent ulcers are certainly non-healing, not all non-healing ulcers are indolent ulcers. Underlying ophthalmic diseases and infection can also prevent ulcers from healing. Therefore, a thorough ophthalmic exam to exclude other diseases that cause persistent ulcers, such as keratoconjunctivitis sicca, distichia, entropion, ectopic cilia, eyelid masses, lagophthalmos (inability to properly blink the eyelids) and ocular foreign bodies is essential before making a diagnosis of an indolent ulcer. Boxers and Corgis are especially predisposed to indolent ulcers, but they can occur in any breed of dog.
Indolent ulcers are most likely caused by trauma, but the exact insult is often never known. The inability of the ulcer to properly heal is due to a number of changes that can be observed on histopathology. These factors are believed to be age-related. The corneal epithelium appears dysplastic and is either unattached or poorly attached to the underlying stroma. A hyalinized aceullar zone is often present in the superficial stroma, and this is the issue that grid keratotomies specifically target. Indolent ulcers are also known to have an abnormal surrounding nerve plexus and mild to moderate suppurative or lymphoplasmacytic inflammation. Unlike melting corneal ulcers, increased levels of matrix metalloproteinases (the corneal enzymes that cause the “melting”) are not present in indolent ulcers, and this is likely why serum is not an effective treatment for them.
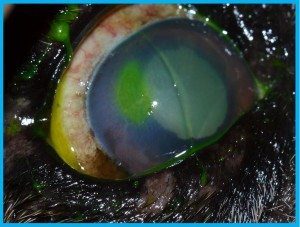
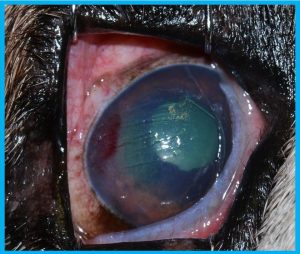
Indolent ulcers have several unique attributes that can be identified on exam. By definition, they are always superficial. If an ulcer appears to involve the corneal stroma or you can see a divot on the cornea, then it is either not an indolent ulcer or it is an indolent ulcer that has become infected and should now be classified as an infected ulcer. In addition, indolent ulcers occur in middle-aged and older dogs with the average age being eight to nine years old. They can occur in dogs as young as 5 years old, though that is uncommon. An indolent ulcer in a dog less than five years old is rare, and other differentials should be strongly considered in that instance. Finally, indolent ulcers typically have a ring of loose corneal epithelium that fluorescein stain can seep under, creating a diffuse stain uptake pattern or a “halo” of stain around the ulcer. As mentioned previously, a thorough ophthalmic exam to exclude other causes of non-healing ulcers is essential.
Indolent ulcers have several unique attributes that can be identified on exam. By definition, they are always superficial. If an ulcer appears to involve the corneal stroma or you can see a divot on the cornea, then it is either not an indolent ulcer or it is an indolent ulcer that has become infected and should now be classified as an infected ulcer. In addition, indolent ulcers occur in middle-aged and older dogs with the average age being eight to nine years old. They can occur in dogs as young as 5 years old, though that is uncommon. An indolent ulcer in a dog less than five years old is rare, and other differentials should be strongly considered in that instance. Finally, indolent ulcers typically have a ring of loose corneal epithelium that fluorescein stain can seep under, creating a diffuse stain uptake pattern or a “halo” of stain around the ulcer. As mentioned previously, a thorough ophthalmic exam to exclude other causes of non-healing ulcers is essential.

Various medical and surgical modalities are used to treat indolent ulcers. The first step is debridement of the loose corneal epithelium with a sterile cotton swab. Generally, normal corneal epithelium cannot be removed with a cotton swab, so any epithelium that is removed is abnormal and considered part of the indolent ulcer. Studies show that cotton swab debridement alone heals an average of 50% of indolent corneal ulcers. When cotton swab debridement is unsuccessful, more aggressive procedures are used.
Diamond burr debridement involves using a dremel-like tool with a spinning bit to debride the ulcer. The exact mechanism for how diamond burrs heal indolent ulcers is unknown, but studies have shown that over 90% of indolent ulcers can heal with this technique.

Grid keratotomies are another essential tool for indolent ulcer management and have an 80% success rate. Superficial scratches are made on the cornea with a 25-gauge needle in a cross-hatch pattern. The scratches should be deep enough that they can be seen, but not so deep that they create deep grooves in the cornea. With noncompliant patients, the last mm of the tip of the needle can be bent 90 degrees with sterile hemostats so that if the needle were to accidentally penetrate the cornea it would avoid lacerating the lens or iris. At our clinic, almost all debridements and grid keratotomies are done using only topical anesthesia with proparacaine and good restraint. Sedation can be useful for clinicians uncomfortable with ophthalmic procedures in conscious patients, but be mindful that it can cause the eye to roll into an unfavorable position. It is not uncommon for a debridement or keratotomy to have to be repeated before an indolent ulcer heals, but it rarely should have to be done more than three times. Placement of a bandage contact lens has been shown in multiple studies to shorten the healing time for indolent ulcers. This may occur due to protection of migrating corneal epithelial cells from the mechanical forces of the eyelids, providing a scaffold for epithelial cells to travel across or increasing contact between the epithelium and underlying stroma. Some studies show an improvement in patient comfort with use of a contact lens.
Less commonly used procedures for indolent ulcers include thermokeratoplasty, application of cyanoacrylate surgical glue to the ulcer and superficial keratectomy. They are rarely used due to the success of the aforementioned procedures. Thermokeratoplasty can be useful for indolent ulcers that are associated with significant corneal edema. Low temperature handheld cautery is used to make numerous punctate superficial burns across the ulcer. The application of excessive heat can cause corneal perforation, so it is best for an ophthalmologist to perform this procedure. The application of cyanoacrylate tissue glue can also be useful in refractory cases, but care has to be taken to avoid gluing the eyelids or third eyelid to the cornea. When none of these modalities work, the last resort option is a superficial keratectomy, or surgical excision of the outermost layer of the corneal ulcer. Keratectomy has a 100% success rate but requires general anesthesia and significant expense compared to the other procedures.
Medically, indolent ulcers should be treated with a topical antibiotic at a frequency of three to four times daily. While a variety of antibiotics can be used, terramycin is our recommendation because it is broad spectrum and has been clinically proven to make indolent ulcers heal faster. This is thought to occur because tetracyclines increase expression of growth factors involved in corneal epithelial cell migration. If terramycin is unavailable, other reasonable options are neopolybac, neopolygram or tobramycin. We do not recommend treating indolent ulcers with topical fluoroquinolones, as those are reserved for infected ulcers. Pain management is also important and can be achieved with oral NSAIDs, tramadol and/or topical atropine. Finally, an e-collar should be worn for the duration of the ulcer. We recommend weekly rechecks until the ulcer has healed. Other medical therapies include artificial tears and topical polysulfated glycosaminoglycans, but these therapies should be used as adjunctive modalities rather than as a substitute for topical antibiotics. Studies have shown that serum is not effective in healing indolent ulcers. Remend has not been shown to specifically heal indolent ulcers, though it may have some benefit as an ocular lubricant.
If you have any questions, please do not hesitate to contact our Ophthalmology service for a consultation. We are happy to help.